Full Digital Documentation for Post Mortem Investigations
MacroVIEW is a comprehensive macro digital imaging system designed to streamline and standardize the documentation of autopsy procedures.
It combines all the necessary tools within a single platform, allowing for the capture of images, recording of audio, and recording of videos of whole bodies, body parts, or large organs.
It combines all the necessary tools within a single platform, allowing for the capture of images, recording of audio, and recording of videos of whole bodies, body parts, or large organs.
-
 Digitalize Autopsy Documentation
Digitalize Autopsy Documentation -
 Legal Evidence for Forensic Investigation
Legal Evidence for Forensic Investigation -
 Remote Viewing and Editing
Remote Viewing and Editing -
 Teaching & Education
Teaching & Education -
 Image-Enchanced Reports
Image-Enchanced Reports
Request a quote
Request a quote


HIGH-RES 4K CAMERA
(up to 20MP) with a 20x optical zoom and 5″ LCD monitor
WATERPROOF 21’’ TOUCHSCREEN
with all functions to capture and store images, videos and audios
HEIGHT ADJUSTABLE CENTRAL COLUMN
with motorized height adjustment and swing arm
INNOVATIVE ANTIMICROBIAL COATING
for easy cleaning and complete disinfection
MOBILE CART
with built-in long-lasting battery
WIDE FIELD OF VIEW
for whole body pictures
196 cm x 110 cm
(77.2’’x 43.3’’)
196 cm x 110 cm
(77.2’’x 43.3’’)
Digitalize Autopsy Documentation
MacroVIEW eliminates the need for using commercial cameras or smartphones for forensic documentation. With its high-resolution camera and user-friendly control terminal, operators can effortlessly capture and store images, record audio, and record videos to support case descriptions. By integrating these tools into a single platform, MacroVIEW enhances workflow, saves time, and improves diagnostic results.

Legal Evidence for Forensic Investigation
Forensic institutes require digital evidence for case filing. MacroVIEW facilitates this process by associating images and videos with the case ID number, enabling full digital documentation for quality control (QC) and quality assurance (QA). It provides digital evidence for forensic and legal investigations, resulting in significant time and cost savings.

Request a Virtual Demo
Request a Virtual Demo

Remote Viewing and Editing
MacroVIEW allows for real-time editing of images during or after the autopsy. The documents can be easily shared through the network (LAN) or integrated into the Laboratory Information System (LIS) or PACS. Pathologists can conveniently view and edit images, measure sizes and surfaces, add text and sections, or create freehand drawings from their office.
Teaching & Education
The high-definition digital material captured during post-mortem examinations serves as valuable educational resources for medical students, residents, and other professionals involved in the field. These materials can be readily used for presentations, conferences, and live-streaming.

Image-Enhanced Reports
MacroVIEW combines all essential tools into a single platform, offering a reliable solution for generating comprehensive IER.
The report includes relevant documentation, which is automatically stored, linked to the case ID number, and easily accessed remotely.
This digitization not only enhances the safety of the procedures, but also standardizes the documentation method, thus contributing to increased efficiency and accuracy in the autopsy process.
This digitization not only enhances the safety of the procedures, but also standardizes the documentation method, thus contributing to increased efficiency and accuracy in the autopsy process.

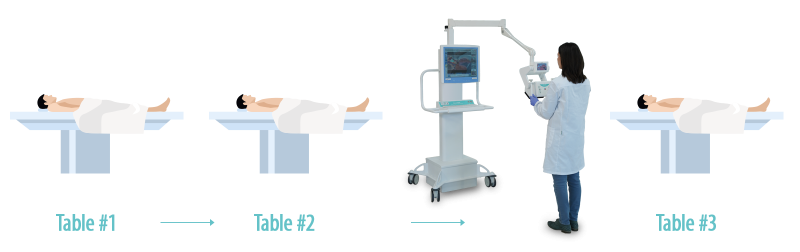
Flexibility
In addition to its superior flexibility during the autopsy process, MacroVIEW can be easily moved across different tables thanks to its built-in, long-lasting battery and complete mobility.